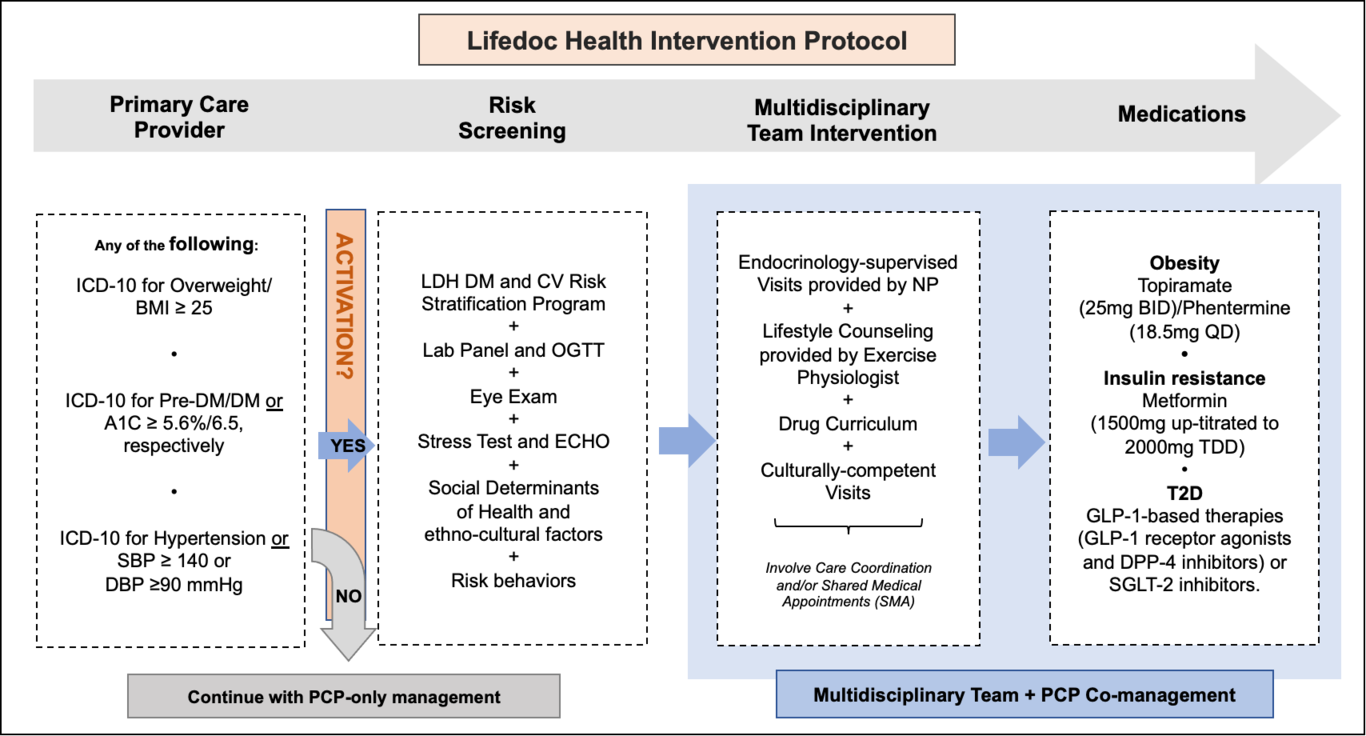
Background: Information regarding the effect of a multidisciplinary team (MDT) to improve cardiometabolic risk factors (CMRF) in routine clinical settings is lacking. Methods: In this one-year retrospective chart review (2018), 598 adults (African American 59%, Hispanic 35%, Caucasian 6%) with a mean age of 43.8 ± 14.0 were included. Qualifying patients (≥ 1 CMRF of overweight/obesity, prediabetes/diabetes, or hypertension) who were treated under an MDT protocol were compared to patients who qualified for MDT but were treated solely by a primary care provider (PCP). The MDT protocol included endocrinology-oriented visits, lifestyle counseling, care coordination, and shared medical appointments. Linear and binary regression were performed to identify the factors associated with CMRF changes. Results: Patients treated by MDT had a greater reduction (β, 95% CI) in weight (- 4.29 kg, -7.62, -0.97), BMI (-1.43 kg/m2, -2.68, -0.18), SBP (- 2.18 mmHg, -4.09, -0.26), and DBP (- 1.97 mmHg, -3.34, -0.60). They also had 77% higher odds of reducing ≥ 5% their initial weight, 83% higher odds of reducing 1 point of BMI, and 59% higher odds of reducing ≥2 mmHg DBP. No association was observed for MDT intervention and A1c changes. Conclusion: Compared to PCP, MDT-protocolized intervention improves CMRF in a multi-ethnic adult cohort in a routine clinical setting. Patient’s activation to access the best care and overcoming barriers from patients (weight perception, social determinants increasing no-shows to visits), providers (obesity stigma, clinical inertia), and health system (time constraints and high paperwork imposed by payers) is a priority.